
Missing Moms
Confounding tilts infant-feeding science toward the breastfeeding ideal. Selection bias removes the mothers who would tilt it back.

A kind nudge from Guido Biele — a research professor at the Norwegian Institute of Public Health who reads more carefully than most — sent me back to the Norwegian Mother, Father and Child Cohort Study (MoBa) and to his 2019 paper on self-selection and loss to follow up. I’d written, in a post on Simpson’s paradox, good luck finding data in which researchers took mothers’ well-being seriously enough to analyze maternal health and breastfeeding problems as confounds in breastfeeding-effect models. He pointed out, fairly, that MoBa comes closer than almost anything else — and then, with admirable honesty, handed me the paper explaining why it still might not be enough.
Read together, the two open up a structural point worth drawing out. Because it changes what “good luck finding data” even means. There are two different biases here, not one — and only one of them is selection bias in the technical sense. I’ve written about the first for years. The second sits underneath it, quieter and more uncomfortable.
Layer 1: Confounding (selection into breastfeeding)
This is the confound I’ve diagrammed before. Maternal health is a fork.
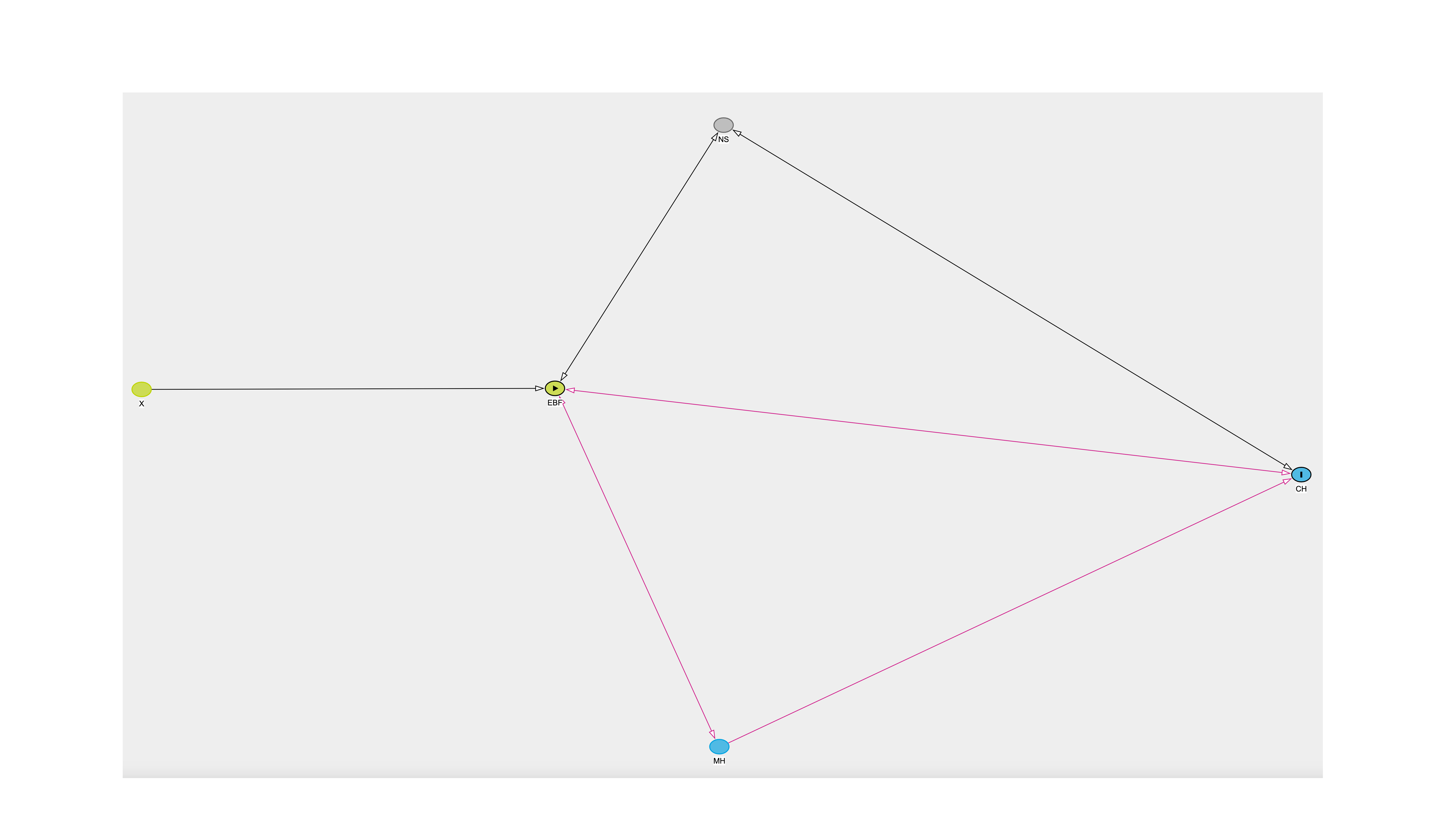
X - Exclusive Breastfeeding Choice
NS - Neonatal Starvation
EBF - Exclusive Breastfeeding
MH - Maternal Health
CH - Child Health
The same biological problems that undermine lactation — inflammation, disordered glucose metabolism, endocrine disorder — can independently raise the risk of postpartum depression.
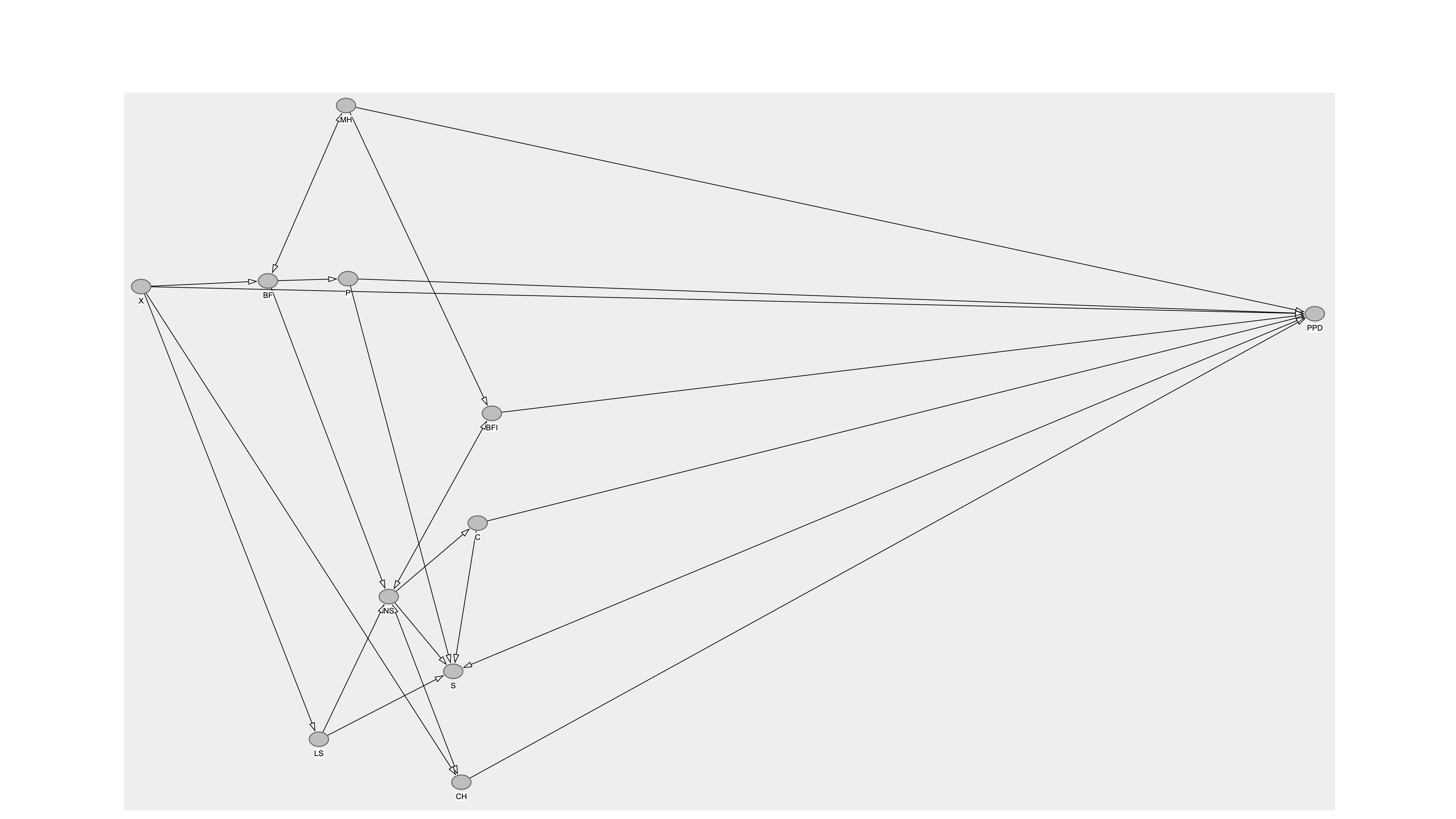
X - breastfeeding choice
BF - breastfeeding
MH - maternal health
BFI - breastfeeding insufficiencies
NS - neonatal starvation
C - excessive infant crying
P - pain
S - sleep deprivation
CH - child health
PPD - postpartum depression
LS - lactation support
Socio-economic status, social support, and stress shape both whether a mother breastfeeds and her odds of depression. So the weak inverse correlations between breastfeeding and PPD that get sold as a protective effect are, at least in part, maternal health sorting women into outcomes. Healthier, better-resourced women breastfeed more and fare better, for reasons that have nothing to do with the milk.
To break this confound, you have to put biology on the board: measure maternal health — really measure it, before the exposure window — and condition on it. That’s hard. But it’s the familiar kind of hard. It’s a confounding problem, and we have tools for confounding problems.
Layer 2: Selection bias (into the observed dataset)
Here is the part Biele’s work made me sit with. Before any of that confounding can bias an estimate, a mother has to be in the sample at all. And who ends up in a cohort like MoBa is anything but random.
Only about 41% of invited women consented — and the ones who did were, on average, older, more educated, and healthier, with fewer health risks, than the ones who didn’t. The cohort over-represents the well, the well-educated, and the well-resourced, and under-represents nearly everyone else. (Typical healthy user bias.) MoBa’s own analysts put it bluntly: it really only supports inference about well-educated Norwegian women without a migration background. (Reading Norwegian was an enrollment requirement.)
Biele et al show, with genetic correlations and inverse-probability-of-participation weighting, that this is no cosmetic problem: for mental health-related exposures and outcomes, the bias from self-selection and attrition is real, and can be practically important (“Bias from self selection and loss to follow‑up in prospective cohort studies,” European Journal of Epidemiology 2019).
Now stack the layers. Maternal education predicts both participation and maternal health. So the confound I most want to study is correlated with the door into the dataset. I am trying to estimate a maternal health-driven relationship inside a sample that has already been filtered on maternal health-adjacent traits. The two mechanisms don’t necessarily politely add. There’s reason to suspect they may compound.
Why the stack is worse than it sounds
Think about which mothers the breastfeeding myth harms most: The ones whose milk is delayed or insufficient. The ones whose babies lose too much weight, or end up back in the hospital for jaundice or dehydration. The ones managing illness, poverty, inadequate social support, no leave, no sleep. The ones for whom “just breastfeed more” is not encouragement but injury and insult with nipple cream on top.
These are precisely the mothers least likely to be in the cohort, and most likely to drop out if they are. The data thins exactly where the counter-evidence lives. The women whose experience would most sharply contradict the claim that breastfeeding protects maternal well-being are selected out of the studies used to defend it.
And here’s the thing: a myth doesn’t do any of this. People do — and mostly what they do is fail to look. No one has to suppress the evidence. The studies were simply built from a world in which that evidence was never collected. Researchers, reviewers, and the institutions that fund them don’t so much ignore the mothers for whom breastfeeding went wrong as never see them. A cohort of educated, well-resourced, mostly-it-went-fine mothers will keep returning the reassuring answer — and the women for whom it wasn’t reassuring aren’t at the table to argue. They’re too busy putting out fires. That’s how a comfortable belief stays comfortable: not by winning the argument, but by never having to have it with the people it hurts.
What it would take
There’s hope for science and society here. The two layers call for two tools, and they’re different tools.
For the confounding layer, you need maternal health measured before the exposure window. MoBa is better here than I’d assumed: symptom checklists and depression history sit in the prenatal waves, and the six-month questionnaire records feeding month by month across the first half-year, so the exposure is finely sliced through exactly the acute window where starvation, jaundice, and pain do their work.
The persistent gap is the biological machinery — delayed lactogenesis, insufficient-milk problems, PCOS, glucose, inflammation — which mostly isn’t in the questionnaires. A little might come from the birth registry or from biobank assays — but because most MoBa births predate the individual-level linkage of Norway’s prescription and patient registries (around 2007-08), that route is largely closed for this cohort. For much of the biological story it’s biobank or nothing, recoverable only with effort, if at all.
For the selection layer, you need something like Biele’s approach: model who got into the sample and weight accordingly, and use genetic correlations to substantiate the assumptions in the causal graph rather than waving at them. That’s how you put the missing mothers back into the estimate — partially, imperfectly, theoretically.
Neither tool substitutes for the other. Weight a sample perfectly, and you’ve still got a maternal health confound. Measure the confound perfectly, and you’ve still got a sample that erased the women it arguably matters for most. You need the DAG for the top layer and the weighting for the bottom one, and you need to say out loud that they interact and that we could be wrong in our modeling assumptions.
The point
“Good luck finding data” was never only about whether the right variables were measured. It was about whether the moms were in the room. Selection bias in this literature isn’t a footnote to the confounding story. It’s the mechanism that lets the confounding story stay comfortable.
We owe new moms and babies a heightened duty of care, and the first clause of that duty is the oldest one: first, do no harm. We cannot honor it with datasets that quietly excused themselves from meeting the people most likely to be harmed by the practices the data are used to support. So if we want science that protects moms and babies instead of flattering a myth that harms both, we have to go looking for the people the data left out — and build the methods that count them anyway.
H/t Guido Biele for the nudges back to MoBa and his excellent 2019 paper.